NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Bookshelf ID: NBK421 PMID: 21250261
Definition
The liver is the largest organ in the human body. During development, liver size increases with increasing age, averaging 5 cm span at 5 years and attaining adult size by age 15. The size depends on several factors: age, sex, body size and shape, as well as the particular examination technique utilized (e.g., palpation versus percussion versus radiographic). By percussion, the mean liver size is 7 cm for women and 10.5 cm for men (Table 94.1). A liver span 2 to 3 cm larger or smaller than these values is considered abnormal. The liver weighs 1200 to 1400 g in the adult woman and 1400 to 1500 g in the adult man.Most if not all of the normal liver is concealed by the right rib cage and is beyond the feel of the examiner's hand (Figures 94.1, 94.2). The normal liver is smooth, with no irregularities. When the liver can be felt, it is usually due to: (1) increased diaphragmatic descent; (2) presence of a palpable caudate or Riedel's lobe; (3) presence of emphysema with an associated depressed diaphragm; (4) thin body habitus with narrow thoracic cage; (5) fatty infiltration (enlarged with rounded edge); (6) active hepatitis (enlarged and tender); (7) cirrhosis (enlarged with nodular irregularity); or (8) hepatic neoplasm (enlarged with rock-hard or nodular consistency).
Technique
The examination is performed with the patient in the recumbent position with the right-handed examiner on the right side of the patient. Every effort should be made to have the patient relaxed to avoid tensing of the abdominal musculature. Flexing of the knees or placing a pillow beneath the knees may facilitate relaxation of the abdominal wall.Initial observation of the abdomen is important, as an enlarged liver may have a visible inferior margin, and the protuberant abdomen harboring ascites may be the first clue to hepatic cirrhosis or malignancy. Other stigmata of liver disease (e.g., vascular spiders or caput medusa) may be observed. The patient's right upper quadrant is observed for the appearance of fullness at rest or on deep inspiration. Auscultation of the liver follows inspection.
Percussion is performed to determine liver size, for the margins of the liver can be estimated by this technique. The upper border is percussed using heavy percussion, eliminating the resonant quality produced by the overlying segment of the lung. Light percussion, with the examiner's ear close to the abdomen, best determines the lower border of the liver, because of the liver's apposition to the anterior abdominal wall. The inferior extent may be underestimated if heavy percussion is used. Percussion should first be performed at the right midclavicular line, then at the midsternal and anterior axillary lines. The normal upper level of the liver is at the level of the right nipple, whereas the lower margin of the liver is at the right costal margin. The normal size is variable, particularly in relation to body size.
Palpation is performed to determine liver shape and consistency. Single-handed palpation is used for lean individuals, while the bimanual technique is best for obese or muscular individuals and for deep palpation. Using either technique, the liver is felt best at deep inspiration.
For single-handed palpation, the examiner's right hand is initially placed below the level of percussed dullness of the inferior liver margin in the midclavicular line parallel to the rectus muscle. This is done so that palpation of the rectus is not confused with palpation of the underlying and adjacent liver. For bimanual palpation (Figure 94.3), the left hand is held posteriorly, between the twelfth rib and the iliac crest, lateral to the paraspinous muscles. It is lifted gently upward to elevate the bulk of the liver into a more easily accessible position, while the right hand is held anterior and lateral to the rectus musculature. The right hand moves upward using gentle, steady pressure until the liver edge is felt.
The normal liver may be slightly tender upon palpation, but the inflamed liver (hepatitis) is often exquisitely tender. The patient should be reassured that such discomfort will be only momentary. The nodularity, irregularity, firmness, and hardness of the liver can be characterized.
Basic Science
Repeated studies have shown that percussion of the liver is superior to the palpatory measurement of liver span below the right costal margin in the estimation of hepatic enlargement. Although palpation and percussion are the most commonly used clinical methods for determining liver size, radiologic methods have recently become popular. Technetium liver scans were favored in the past but often underestimated liver size, particularly in metastatic disease. Ultrasound is fairly accurate, but computed tomography is the most reliable method of determining vertical liver span and overall dimensions.With the advent of liver transplantation, it has become clear that there is a great need for an exact determination of liver size. Calculated volume measurements made at ultrasound or at computed tomography provide the best estimates. With computed tomography, 8 to 12 serial transverse slices are obtained, the enclosed area is calculated by computer, and the total organ volume is estimated. This technique provides calculated liver volumes within 5% of the actual volume as determined at autopsy. A recent report using sagittal sections of the liver obtained by ultrasound was found to be superior to transverse sections obtained with computed tomography because of the lack of respiratory artifact when sagittal sections are obtained. Further refinements of these and other scanning techniques may increase accuracy.
Clinical Significance
In the majority of normal examinations the liver is not palpable. Cases in which the normal liver is palpable include emphysema, right-sided pleural effusion, thin body carriage, Riedel's lobe, or deep diaphragmatic excursion.In emphysema, the lungs are hyperexpanded with diaphragmatic flattening, thereby lowering the upper and lower borders of the liver. A large right pleural effusion will have the same effect of lowering the liver boundaries. Accurate percussion of the upper liver border in a patient with a right pleural effusion can be difficult because of the fluid density overlying liver dullness. Persons with deep diaphragmatic excursion, such as singers and endurance athletes, may have a palpable liver on inspiration.
The most common diseases (Table 94.2) associated with a palpable and enlarged liver include metastatic cancer, lymphoma, congestive heart failure, alcoholic hepatitis, and other causes of fatty liver (e.g., jejunoileal bypass and total parenteral nutrition). Cirrhosis may be associated with a liver of small, normal, or enlarged size.
In metastatic or primary liver cancer, the liver becomes infiltrated with deposits of cancer cells that can grow rapidly. Such neoplastic growth can usually be distinguished from normal liver by palpation of hard and/or nodular tissue consistency. Similar liver enlargement can occur in lymphoma. In cirrhosis, the liver may be enlarged or small, the latter usually occurring in end-stage cirrhosis or fulminant hepatic failure following hepatocyte necrosis and collapse. The consistency is usually nodular in cirrhosis. Classically it is micronodular due to alcoholic or nutritional disease and macronodular when cirrhosis is posthepatitic. Alcoholic hepatitis and other causes of fatty liver lead to liver enlargement by hepatocyte fatty infiltration and hepatocyte enlargement. Hepatic distention and smooth enlargement are typical of significant right-sided heart failure, which occurs because of hepatic venous congestion secondary to impaired myocardial function.
References
- Castell DO, Frank BB. Abdominal examination: role of percussion and auscultation. Postgrad Med. 1977;62(6):133. [PubMed: 928243]
- Castell DO, O"Brien DK, Myench H, Chalmers TC. Estimation of liver size by percussion in normal individuals. Ann Intern Med. 1969;70:1183–89. [PubMed: 5795743]
- Delp MH, Manning RT. Major's physical diagnosis. Philadelphia: W. B. Saunders. 1968;209–15.
- Henderson JM, Heymsfield SB, Horowitz J, Kutner MH. Measurement of liver and spleen volume by computed tomography. Radiology. 1981;14:525–27. [PubMed: 6974875]
- Levitt RE, Roth JLA. General physical examination, Vol 1. Clinical evaluation. Gastroenlerology (Bockus). Philadelphia: W. B. Saunders. 1985;257–275.
- Netter FH. Digestive system. Part III: Liver, biliary tract, and pancreas. The Ciba Collection of Medical Illustrations. Summit, N.J.: Ciba Pharmaceutical, 1964;4–5.
- Prior JA, Silbenstein JS, Stang JM. Physical diagnosis. St. Louis: C. V. Mosby, 1981;310–19.
- Van Thiel DH, Hagler NG, Schade RR. et al. In vivo volume determination using sonography and computed tomography. Gastroenterology. 1985;88:1812–17. [PubMed: 3888769]
Figures
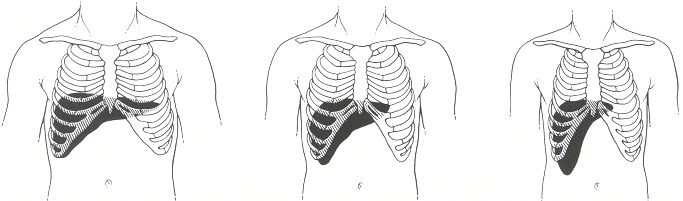
Figure 94.1
Frontal views of the liver for different body types. (Source: Castell DO, Frank BB. Abdominal examination: role of percussion and auscultation. Postgrad Med 1977;62(6): 133. Reproduced with permission.)
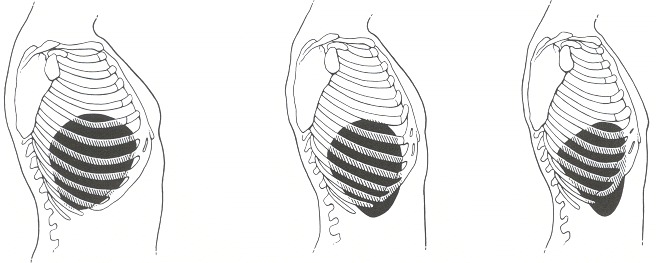
Figure 94.2
Lateral views of the liver for different body types. (Source: Castell DO, Frank BB. Abdominal examination: role of percussion and auscultation. Postgrad Med 1977;62(6): 133. Reproduced with permission.)
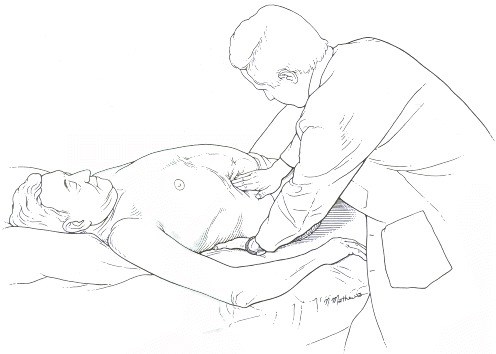
Figure 94.3
Bimanual technique for palpation of liver.
Tables
Table 94.1Average Liver Span by Percussion in Normal Individuals
| Liver dullness (cm) | ||||
|---|---|---|---|---|
| Midclavicular line | Midsternal line | |||
| Height (in) | Men | Women | Men | Women |
| 60 | 8.25 | 6.00 | 6.00 | 4.00 |
| 63 | 9.00 | 6.75 | 6.50 | 4.50 |
| 66 | 9.75 | 7.50 | 7.00 | 5.00 |
| 69 | 10.25 | 8.00 | 7.50 | 5.50 |
| 72 | 11.00 | 8.75 | 8.00 | 5.75 |
| 75 | 11.75 | 9.50 | 8.50 | 6.25 |
- Source: Castell DO, Frank BB. Abdominal examination: role of percussion and auscultation. Postgrad Med 1977;62(6): 131–34. Reproduced with permission.
Table 94.2Examination Findings Associated with Specific Liver Diseases
| Liver disease | Palpation | Size |
|---|---|---|
| Acute hepatitis | Smooth; surface tender | Enlarged |
| Chronic hepatitis | Firm liver edge | Enlarged, especially left lobe |
| Nodules rare; tender | ||
| Fulminant hepatitis | Tender surface | Shrinking size |
| Cirrhosis | Nontender, firm | Variable; late stages, liver decreases in size |
| Hepatocellular carcinoma (hepatoma) | Nodules, if present, large and hard | Moderate to massive enlargement |
| Nontender | ||
| Metastatic carcinoma | Large nodules | Enlarged |
| Nontender | ||
| Fatty liver | Smooth surface | Enlarged |
| Right heart failure | Firm, smooth, tender | Mild to massive enlargement |
Copyright © 1990, Butterworth Publishers, a division of Reed Publishing.
Nice blog and absolutely outstanding. You can do something much better but i still say this perfect.Keep trying for the best.
Trả lờiXóaলিভার ভালো রাখার খাবার