NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Bookshelf ID: NBK420 PMID: 21250260
Definition
Inspection consists of visual examination of the abdomen with note made of the shape of the abdomen, skin abnormalities, abdominal masses, and the movement of the abdominal wall with respiration. Abnormalities detected on inspection provide clues to intra-abdominal pathology; these are further investigated with auscultation and palpation.Auscultation of the abdomen is performed for detection of altered bowel sounds, rubs, or vascular bruits. Normal peristalsis creates bowel sounds that may be altered or absent by disease. Irritation of serosal surfaces may produce a sound (rub) as an organ moves against the serosal surface. Atherosclerosis may alter arterial blood flow so that a bruit is produced.
Palpation is the examination of the abdomen for crepitus of the abdominal wall, for any abdominal tenderness, or for abdominal masses. The liver and kidneys may be palpable in normal individuals, but any other masses are abnormal.
Technique
Inspection
The abdomen is inspected by positioning the patient supine on an examining table or bed. The head and knees should be supported with small pillows or folded sheets for comfort and to relax the abdominal wall musculature. The entire abdominal wall must be examined and drapes should be positioned accordingly. The patient's arms should be at the sides and not folded behind the head, as this tenses the abdominal wall. Good lighting is essential, and it is helpful to have tangential lighting available, for this can create subtle shadows of abdominal wall masses.First, the general contour of the entire abdominal wall is observed. The contour should be checked carefully for distention and note made as to whether any distention is generalized or localized to a portion of the abdomen. Similarly, the flanks should be checked for any bulging.
The abdominal wall skin should be inspected carefully for abnormalities. Any areas of discoloration should be noted, such as the bluish discoloration of the umbilicus (Cullen's sign) or flanks (Grey Turner's sign). The skin should be inspected for striae, or "stretch marks," and surgical scars. Careful note of surgical scars should be made and correlated with the patient's recollection of previous operations. The skin of the abdomen should also be checked carefully for engorged veins in the abdominal wall and the direction of blood flow in these veins. This is performed by placing the tips of the index fingers together, compressing a visible vein. The fingertips are then slid apart, maintaining compression, producing an empty venous segment between the fingers. A finger is removed from one end and the vein is watched for filling. The procedure is then repeated, but the opposite finger is removed and the vein again checked for filling. Above the umbilicus, blood flow is normally upward; below the umbilicus, it is normally downward. Obstruction of the inferior vena cava will cause reversal of flow in the lower abdomen. In addition to these large dilated veins, note should be made of any spider angiomas of the abdominal wall skin.
Next, the abdomen should be inspected for masses. This should be performed from several angles. It is important to differentiate abdominal wall from intra-abdominal masses. A mass of the abdominal wall will become more prominent with tensing of the abdominal wall musculature, whereas an intra-abdominal mass will become less prominent or disappear. Useful maneuvers are to have the patient hold his head unsupported off the examining table, to hold his nose and blow, or to raise his feet off the table. Abdominal wall masses are most commonly hernias (either umbilical, epigastric, incisional, or spigelian), neoplasms (benign and malignant), infections, and hematomas.
Once a mass is determined to be intra-abdominal, its location should be described in relation to the abdominal quadrants (Figure 93.1). The relationship of intra-abdominal organs to these quadrants should be considered in attempting to determine the cause of the mass. The mass should be examined for movement with respiration or for pulsation with each heartbeat. Also, the mass should be observed for peristalsis, as it may well represent dilated bowel.
Lastly, the abdominal wall should be observed for motion with respiration. Normally, the abdominal wall moves posteriorly in a symmetrical fashion with inspiration. With peritonitis, there may be localized or generalized rigidity of the abdominal wall so that this motion is absent.
Auscultation
The patient is positioned comfortably in the supine position as described in Inspection. The stethoscope is used to listen over several areas of the abdomen for several minutes for the presence of bowel sounds. The diaphragm of the stethoscope should be applied to the abdominal wall with firm but gentle pressure. It is often helpful to warm the diaphragm in the examiner's hands before application, particularly in ticklish patients. When bowel sounds are not present, one should listen for a full 3 minutes before determining that bowel sounds are, in fact, absent.Auscultation for abdominal bruits is the next phase of abdominal examination. Bruits are "swishing" sounds heard over major arteries during systole or, less commonly, systole and diastole. The area over the aorta, both renal arteries. and the iliac arteries should be examined carefully for bruits.
Rubs are infrequently found on abdominal examination but can occur over the liver, spleen, or an abdominal mass.
Palpation and Percussion
The patient is positioned supine with head and knees supported, as for Inspection and Auscultation. Take the history and perform inspection and auscultation before palpation, as this tends to put the patient at ease and increases cooperation. In addition, palpation may stimulate bowel activity and thus falsely increase bowel sounds if performed before auscultation. Ask patients with abdominal pain to point to the area of greatest pain. Then reassure them that you will try to minimize their discomfort and examine that point last.In palpating the abdomen, one should first gently examine the abdominal wall with the fingertips. This will demonstrate the crunching feeling of crepitus of the abdominal wall, a sign of gas or fluid within the subcutaneous tissues. In addition, it will demonstrate any irregularities of the abdominal wall (such as lipomas or hernias) and give some idea as to areas of tenderness.
Deep palpation of the abdomen is performed by placing the flat of the hand on the abdominal wall and applying firm, steady pressure. It may be helpful to use two-handed palpation (Figure 93.2), particularly in evaluating a mass. Here the upper hand is used to exert pressure, while the lower hand is used to feel. One should start deep palpation in the quadrant directly opposite any area of pain and carefully examine each quadrant. At each costal margin it is helpful to have the patient inspire deeply to aid in palpation of the liver, gallbladder, and spleen.
In the flanks it is often helpful to elevate the flank to be examined slightly and place one hand on the lower ribs of that flank to "push" the retroperitoneal contents up to the examining hand. In this way, small renal masses that would otherwise be missed may be appreciated.
Abdominal tenderness is the objective expression of pain from palpation. When elicited, it should be described as to its location (quadrant), depth of palpation required to elicit it (superficial or deep), and the patient's response (mild or severe). Spasm or rigidity is the involuntary tightening of the abdominal musculature that occurs in response to underlying inflammation. Guarding, in contrast, is a voluntary contraction of the abdominal wall musculature to avoid pain. Thus, guarding tends to be generalized over the entire abdomen, whereas rigidity involves only the inflamed area. Guarding can often be overcome by having the patient purposely relax the muscles; rigidity cannot be. Rigidity is thus a clear-cut sign of peritoneal inflammation.
Rebound tenderness is the elicitation of tenderness by rapidly removing the examining hand. Again, this is a difficult sign for the beginning examiner to master. The most common error is to remove the hand very quickly with an exaggerated motion and thus startle the patient. All that needs to be done is smoothly but quickly to lift the palpating hand off the abdomen and observe for pain, facial grimace, or spasm of the abdominal wall. Both tenderness and rebound tenderness may be elicited by palpation in a different quadrant. Thus, palpation of the left lower quadrant may produce tenderness and rebound tenderness in the right lower quadrant in appendicitis (Rovsing's sign). This is called referred tenderness and referred rebound.
When abdominal masses are palpated, the first consideration is whether the mass is intra-abdominal or within the abdominal wall. This can be determined by having the patient raise his or her head or feet from the examining table. This will tense the abdominal muscles, thus shielding an intra-abdominal mass while making an abdominal wall mass more prominent. If the mass is intra-abdominal, important points are its size, location, tenderness, and mobility.
Palpation and percussion are used to evaluate ascites. A rounded, symmetrical contour of the abdomen with bulging flanks is often the first clue. Palpation of the abdomen in the patient with ascites will often demonstrate a doughy, almost fluctuant sensation. In advanced cases the abdominal wall will be tense due to distention from the contained fluid. Gas-filled intestines will float to the top of the fluid-filled abdomen. Thus, in the supine patient with ascites there should be periumbilical tympany with dullness in the flanks. One should mark the level of dullness on the skin and then turn the patient on one side for a full minute. A change in the level of dullness is termed shifting dullness and usually indicates more than 500 ml of ascitic fluid. Another physical sign of ascites is demonstration of a transmitted fluid wave. The patient or an assistant presses a hand firmly against the abdominal wall in the umbilical region. The examiner places the flat of the left hand on the right flank and then taps the left flank with his right hand. In the presence of ascites, a sharp tap will generate a pressure wave that will be transmitted to the left hand. Unfortunately, fat will also transmit a fluid wave, and there are frequent false-positives with this test.
In addition to detection of ascites, percussion can be used to help define the nature of an abdominal mass. Tympany of an abdominal mass implies that it is gas filled (i.e., intestine). Percussion is also used to define liver size.
Basic Science
Normal peristalsis of the intestine produces bowel sounds as gas and fluid are passed through the intestinal lumen. Normally, the bowel sounds are intermittent, low-pitched, chuckling sounds. Bowel sounds may be decreased or increased in disease states.Ileus is a failure of peristalsis and is the normal physiologic response of the intestine to laparotomy or peritoneal inflammation. In addition, ileus is seen in a number of disease states that do not affect the peritoneum directly, including pneumonia, congestive heart failure, and uremia. Bowel sounds will be markedly diminished or absent in ileus as the intestine distends with gas in its paralyzed state.
Early mechanical bowel obstruction produces hyperactive peristaltic waves proximal to the mechanical obstruction. These waves are increased in frequency and force and produce a concomitant increase in bowel sounds with characteristic "rushes." As the bowel gradually dilates with gas and fluid, the bowel sounds become high pitched and tinkling, and there may be periods of hypoactive bowel sounds that alternate with hyperperistaltic rushes. These rushes correlate with the increased peristaltic activity. Finally, in late intestinal obstruction there may be loss of all bowel sounds due to loss of peristaltic activity from vascular compromise.
Vascular bruits are the audible manifestation of turbulent blood flow. They are found normally in thin patients, but in heavier individuals will be muffled because of the surrounding fat. Loud systolic bruits are due to atherosclerotic plaques within arteries, producing turbulent flow. These plaques are common in the aorta and iliac arteries and less common in the renal arteries. In addition, turbulent flow within an abdominal aortic aneurysm may create a bruit. Bruits that are present in both systole and diastole are strongly suggestive of an arteriovenous communication.
Rubs are uncommon on abdominal auscultation but, when found, are the result of inflamed peritoneal surfaces grating on each other during respiration. This can be the result of a neoplastic or infectious process that destroys the normally smooth peritoneal surfaces.
Crepitus is produced by gas (air) and/or fluid within tissues. In the abdominal wall, it either is due to traumatic introduction of air or is secondary to infection (gas gangrene). Subcutaneous emphysema can occur from rupture of a pulmonary bleb or penetrating chest injury with dissection of air into the subcutaneous spaces. In addition, penetrating abdominal trauma may introduce enough air into the abdominal wall to produce crepitus. Gas gangrene can occur as a complication of intra-abdominal surgery and produce crepitus of the abdominal wall. The gas is produced by anaerobic bacteria (usually clostridia species) and is a very specific clinical sign when found in the patient with wound infection.
Abdominal tenderness occurs as a result of irritation of the parietal peritoneum. While inflammation or irritation of the visceral peritoneum will cause abdominal discomfort, anorexia, and poorly localized pain, it will not cause tenderness and rigidity of the abdominal wall. Irritation or inflammation of the parietal peritoneum will stimulate the pain fibers of the parietal peritoneum and abdominal wall, creating the symptoms of localized pain and the signs of tenderness, rigidity, and rebound tenderness. Thus, if there is diffuse irritation of the peritoneum, as in diffuse peritonitis, there will be diffuse tenderness and rigidity.
Abdominal masses arise from the surrounding structures, thus the importance of topographic relationships. The presence or absence of tenderness of a mass gives important information as to its etiology. An appendiceal abscess will be tender as it inflames the parietal peritoneum, whereas carcinoma of the cecum will be nontender because there is no inflammation involved. Tympany over a mass implies it is gas filled. In the abdomen, this usually signifies the mass is dilated bowel, as only rarely will there be enough gas in any other mass to produce tympany.
Ascites is the presence of intra-abdominal fluid and occurs because of overproduction of intra-abdominal fluid or lack of absorption. It is most commonly seen in cirrhosis in which there is an increase in portal pressure and hypoalbuminemia. The increased portal pressure hydrostatically increases transudation of fluid through capillaries, whereas the hypoalbuminemia hydrostatically favors ascites formation. Thus, there is accumulation of fluid in the peritoneal space, which signifies severe liver disease. Other common causes of ascites include carcinomatosis in which there is both an increase in fluid formation and difficulties in clearing intraperitoneal fluid, and congestive heart failure in which there is a hydrostatic increase in venous pressure.
Clinical Significance
Inspection
Inspection of the abdomen gives clues to the diagnosis of intra-abdominal pathology. Combined with the patient's history, inspection can often provide a preliminary diagnosis that can be confirmed by auscultation and palpation. Despite the current popularity of various noninvasive and invasive diagnostic tests, the experienced surgeon can usually make an accurate diagnosis of intra-abdominal pathology by history and physical examination. This is demonstrated by the patient with a several-day history of right upper quadrant and back pain with associated nausea, vomiting, fever, and a visible mass in the right upper quadrant. Such a patient almost certainly has acute cholecystitis with hydrops of the gallbladder. The remainder of the physical examination merely confirms this and detects additional disease. Though inspection alone never provides a clear diagnosis, it should not be overlooked.Generalized distention of the abdomen is usually from obesity, bowel distention by gas or liquid, or ascites. Obesity can cause generalized distension by either fat in the abdominal wall or intra-abdominal fat in the omentum or viscera. Generalized abdominal distention can also be related to ascites, particularly when associated with an everted umbilicus. Distention of the upper half of the abdomen only may be due to pancreatic cyst or tumor or to acute gastric dilatation. Distention of the lower half of the abdomen may be due to pregnancy, ovarian tumor, uterine fibroids, or bladder distention. A scaphoid abdomen is due to malnutrition.
Skin abnormalities detected on inspection of the abdominal wall need to be correlated with the clinical history. Bruising should be correlated with a history of trauma to determine the possible organs injured. Cullen's and Grey Turner's signs (bluish discoloration of the umbilicus and flanks, respectively) are related to intra-abdominal and retroperitoneal bleeding, and it is believed the blood dissects along fascial planes to reach these areas. Thus, one would want to question the patient diligently for causes of such bleeding—severe pancreatitis, trauma, or ruptured ectopic pregnancy.
Striae of the abdominal wall are a result of rupture of the reticular dermis that occurs with stretching. This is seen clinically in pregnancy, obesity, ascites, abdominal carcinomatosis, and Cushing's syndrome.
Surgical scars should be examined carefully, both as to their position and their characteristics. Often patients are unsure of what kinds of surgery they have had, but the position of the incision may give the examiner a clue. Even though a transverse right lower quadrant incision suggests appendectomy, however, it in no way proves it, and one must be circumspect in making any such assumptions. The scar tells the examiner about the surgery. All scars are initially raised and red; they gradually fade to pink and by 6 months are generally flat and skin colored or gray. Wounds that heal cleanly by first intention are thin and regular, whereas those that are infected and heal by secondary intention are wider and irregular. Keloids are wide, irregular scars with abundant hypertrophic tissue outside the field of normal scarring. Keloid formation tends to recur in certain individuals and is particularly common in blacks.
Enlarged veins are seen in three clinical situations: emaciation, portal hypertension, and inferior vena cava obstruction. In emaciation there is loss of subcutaneous fat so that the normally invisible veins become prominent. These veins become more prominent in the presence of portal hypertension. In portal hypertension the umbilical vein becomes an outflow tract of the portal system and forms collaterals with the veins of the abdominal wall. This is responsible for the caput medusa that is diagnostic of portal hypertension. The direction of blood flow in these veins in portal hypertension is normal (i.e., upward in those above the umbilicus and downward in those below) as the blood is flowing from the high-pressure portal system to the low-pressure systemic system. Finally, the veins of the abdominal wall may be dilated due to obstruction of the inferior vena cava. This occurs because the abdominal wall becomes a collateral, or bypass, around the obstruction of the cava. In this situation the direction of blood flow will be reversed below the umbilicus as the blood flows from the femoral vein to the superior vena cava. Obstruction of the inferior vena cava can occur as a result of a hepatic malignancy, as an extension of hepatic vein obstruction (Budd–Chiari syndrome), as a result of thrombophlebitis, or as a result of trauma or surgical intervention.
Masses noted on inspection of the abdomen may be related to organs in that area. Thus, a mass in the right upper quadrant may represent hepatomegaly from hepatitis or hepatic tumor, a distended gallbladder from cholecystitis or pancreatic cancer, or a carcinoma in the head of the pancreas. An epigastric mass is likely to be from acute gastric distention. pancreatic pseudocyst, pancreatic cancer, or aneurysm of the abdominal aorta (which will be pulsatile). Masses in the left subcostal region are generally due to splenomegaly, although carcinoma of the spenic flexure of the colon is also a possibility.
Masses in the lumbar region are generally of renal origin. Renal cysts, polycystic kidneys, and renal malignancies may all be visible in asthenic patients.
Masses in the lower quadrants may result from inflammatory or neoplastic disorders of the intestine. In the right lower quadrant appendiceal abscess and cecal carcinoma are most likely, while in the left lower quadrant diverticular abscess or carcinoma of the sigmoid colon is most likely.
Hypogastric masses are the result of pelvic pathology. Acute urinary retention is the most common cause of such a mass in males. In females, uterine or ovarian neoplasms may cause visible midline abdominal masses.
Visible intestinal peristalsis is usually the result of intestinal obstruction. This can be seen in the stomach of the newborn with hypertrophic pyloric stenosis and in the small intestine of patients with small bowel obstruction from various etiologies.
Auscultation
Bowel sounds are of significance to the clinician as a marker of intra-abdominal pathology. The absence of bowel sounds may be one of the few indicators of intra-abdominal infection in patients with multiple problems and, particularly, altered mental status. In patients with generalized abdominal distention following laparotomy, bowel sounds may be the key diagnostic finding to differentiate ileus from early postoperative small bowel obstruction. Though radiographic examination of the abdomen may suggest bowel obstruction, the characteristic high-pitched bowel sounds are diagnostic for the experienced clinician.Similarily, vascular bruits are helpful to the clinician as an indicator of underlying pathology. Thus they should be carefully searched for in patients with hypertension (renal artery stenosis), chronic abdominal pain (mesenteric arterial insufficiency), or claudication (occlusive disease of the aorta or iliac arteries). As continuous bruits are caused by arteriovenous fistulas, they should be searched for carefully in patients with penetrating abdominal trauma.
Abdominal rubs are rare, but may be found over the liver or spleen. A rub implies that the surface of the organ is irregular and usually is due to involvement by tumor, abscess, or infarction. More rarely, an inflammatory intra-abdominal mass may have an associated rub caused by irritation of the adjacent abdominal wall.
Palpation and Percussion
As mentioned previously, abdominal tenderness is a difficult physical finding to master. Nevertheless, it is a finding that must be mastered because it is often the only clear finding in peritonitis and may well determine therapy. The classic example of this is appendicitis. The history and laboratory findings may suggest appendicitis in a patient with abdominal pain, but the presence or absence of tenderness makes or breaks the diagnosis. As there are no laboratory studies that can either exclude or ensure the diagnosis of appendicitis, the clinician must make therapeutic decisions based on the physical finding of tenderness.As tenderness is caused by inflammation of the parietal peritoneum, the etiology of tenderness can be related to the underlying organs. Thus, right upper quadrant tenderness may be caused by cholecystitis, ulcer disease, pancreatitis, or hepatitis. Epigastric tenderness is usually due to pancreatitis or peptic ulcer disease. Right lower quadrant tenderness may be related to appendicitis, cecal diverticulitis, or perforated carcinoma, whereas left lower quadrant tenderness is usually due to sigmoid diverticulitis. Flank tenderness is usually related to renal pathology, either pyelonephritis or perinephric abscess.
When tenderness is generalized, one must consider causes for generalized peritonitis. Acute perforated ulcer is a frequent cause and presents with characteristic "boardlike" rigidity of the abdominal wall. Other common causes include perforated diverticulitis, perforated appendicitis, and pancreatitis. Nevertheless, any process that produces generalized peritoneal irritation (chemical or infectious) will produce the same physical findings.
Abdominal masses are related to the underlying organs. Right upper quadrant masses include hepatomegaly, hydrops of the gallbladder, and carcinoma of the head of the pancreas. Epigastric masses are pancreatic (pseudocyst or carcinoma), gastric malignancies, and colon malignancies. Masses in the left upper quadrant are usually due to either splenomegaly or carcinoma of the stomach or colon. In the flanks, masses usually arise from the kidney (cyst or tumor), although occasionally from other retroperitoneal structures (lymphoma, sarcoma). Masses in the lower quadrants usually arise from the bowel. On the right side, common masses include appendiceal abscess and cecal carcinoma; on the left, diverticular abscess and sigmoid carcinoma. Central abdominal masses are often aortic aneurysms, and the pulsatile nature of the mass is diagnostic. Thus, in evaluating an abdominal mass, one must consider its location, mobility, and the presence or absence of tenderness in order to define its etiology.
The clinical significance of ascites is based largely on its etiology. This can often be determined by the history and physical examination, but paracentesis is diagnostic. Samples of peritoneal fluid should be sent to the laboratory for protein concentration, specific gravity, cell counts, and culture. Exudative ascites occurs in bacterial peritonitis, carcinomatosis, and pancreatic ascites and is associated with a protein concentration of over 3 gm/dl and a specific gravity above 1.016. Transudative ascites occurs in cirrhosis, Budd–Chiari syndrome, constrictive pericarditis, congestive heart failure, and hypoalbuminemic disorders such as the nephrotic syndrome. In these incidences the protein concentration is less than 3 gm/dl and the specific gravity less than 1.016.
References
- Bailey H. Demonstrations of physical signs in clinical surgery. 13th ed. Baltimore: Williams and Wilkins, 1960.
- Cope Z. The early diagnosis of the acute abdomen. 14th ed. London: Oxford University Press, 1972.
Figures
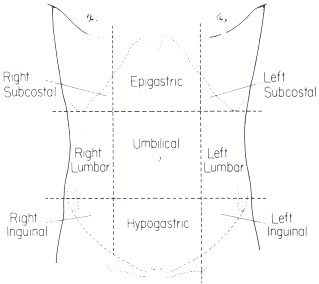
Figure 93.1
Anatomical areas of the anterior abdominal wall.
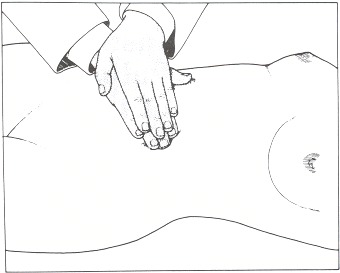
Figure 93.2
Two-handed deep palpation.
Copyright © 1990, Butterworth Publishers, a division of Reed Publishing.
Hiv disease for the last 3 years and had pain hard to eat and cough are nightmares,especially the first year At this stage, the immune system is severely weakened, and the risk of contracting opportunistic infections is much greater. However, not everyone with HIV will go on to develop AIDS. The earlier you receive treatment, the better your outcome will be.I started taking ARV to avoid early death but I had faith in God that i would be healed someday.As a Hiv patient we are advise to be taking antiretroviral treatments to reduce our chance of transmitting the virus to others , few weeks ago i came on search on the internet if i could get any information on Hiv treatment with herbal medicine, on my search i saw a testimony of someone who has been healed from Hiv her name was Achima Abelard and other Herpes Virus patient Tasha Moore also giving testimony about this same man,Called Dr Itua Herbal treatment.I was moved by the testimony and i contacted him by his Email.drituaherbalcenter@gmail.com . We chatted and he send me a bottle of herbal medicine I drank it as he instructed me to.After drinking it he ask me to go for a test that how i ended my suffering life of Hiv patent,I'm cured and free of Arv Pills.I'm forever grateful to him Doctor Itua Herbal Treatment..He assured me he can cure the following disease..Hiv,Cancer,Herpes Virus,Hpv,Pile,Weak Erection,Lyme Disease,Epilepsy,Glaucoma.,Brain Tumor,psoriasis, Cataracts,Macular degeneration,Cardiovascular disease,Chronic Diarrhea,Lung disease.Enlarged prostate,Osteoporosis.Alzheimer's disease,
Trả lờiXóaDementia. ,Bladder Cancer,Autism,Colorectal Cancer,Breast Cancer,Kidney Cancer,Leukemia,Lung Cancer,Tay tach disease,Non Hodgkin Lymphoma,Skin Cancer,Lupus,Uterine Cancer,Prostate Cancer, Seizures, fibromyalgia ,ALS,Hepatitis,Copd,Parkinson disease.Genetic disease,Fibrodysplasia disease,Fibrodysplasia Ossificans Progressiva,Fluoroquinolone Toxicity Syndrome,Stroke,Hpv,Weak Erection,Liver/Kidney Inflammatory,Men/Woman infertility, bowel disease ,Huntington's disease ,Diabetes,Fibroid.