NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Bookshelf ID: NBK418 PMID: 21250258
Definition
The American Psychiatric Association (DSM-III, 1980) has defined alcoholism and alcohol abuse as follows: alcoholism (or alcohol dependence) is "either a pattern of pathological alcohol use or impairment in social or occupational functioning due to alcohol, and either tolerance or withdrawal." A simplified interpretation of this definition is presented in Figure 91.1. Alcohol abuse is defined as "a pattern of pathological use for at least a month that causes impairment in social and occupational functioning."Few definitions in medicine have incited as much discussion as that of "alcoholism," mainly because excessive drinking may manifest as a medical problem (e.g., withdrawal seizures), a psychiatric problem (e.g., depression), or a social problem (e.g., involvement in an automobile accident). On the other hand, a person with a single episode of an alcohol-related problem is not necessarily an alcoholic; in such a case, the condition may be better termed "alcohol abuse."
Technique
It is essential to obtain a detailed drinking history from all patients, since alcohol abuse is widespread among males and females of all occupations and all ages from adolescence onward. The astute physician must always suspect alcohol abuse as the possible underlying cause of a wide variety of common complaints such as fatigue, depression, headaches, heartburn, or palpitations.Very often, the diagnosis of either alcoholism or alcohol abuse can be made with confidence on the basis of the medical history alone. However, the detection of alcohol-induced pathology may require a complete physical examination and laboratory tests. It is beyond the scope of this chapter to discuss these investigations in detail, but the clinician should be alert for such signs as an "alcoholic smell" of the breath, cutaneous signs such as facial erythema, spider hemangiomas, palmar and plantar erythema, and features of hepatic disease such as jaundice, hepatomegaly, Dupuytren's contracture, and edema.
The alcohol drinking history should elicit the average amount of alcohol consumed each day, the pattern of the patient's drinking (relative to time and events), and the impact of this drinking on the patient's social well-being, work, and physical health.
Quantity of Alcohol Consumed
Patients who drink alcohol to excess are prone to feel guilty and then defensive when asked about their consumption and frequently give misleading answers. It is often best to avoid direct confrontational questions like "How much alcohol do you drink?" More effective is a sequence of questions starting with frequency and location of drinking and culminating in quantity (Table 91.1). It is often illuminating to use these figures to calculate an estimated daily dosage of ethanol per unit of body weight, using the formula:
Example: A 150-pound man drinks a pint of scotch whiskey a day. His usual brand is 100 proof (i.e., 50% ethanol by volume).




Social Effects of Drinking
It is important to determine if the patient's social life has been at all disrupted by the consumption of alcohol. The four questions of the CAGE test provide a useful and rapid screen for the adverse social effects of drinking (CAGE is an acronym for Concern, Anger, Guilt and Eye-opener):- Are you concerned about your drinking?
- Do you get angry if anyone criticizes your drinking?
- Do you feel guilty about your drinking?
- Do you ever take an eye-opener? (i.e., a drink in the morning)
In one study of the CAGE test, 81% of known alcoholics answered two or more of these questions affirmatively, compared with only 11% of nonalcoholics (Mayfield et al., 1974). However, even a single affirmative response should arouse suspicions of problems with alcohol.
The patient should be asked if alcohol drinking has had any adverse effects upon his or her work, particularly:
- Have you ever missed work because of your drinking? (e.g., Monday morning absenteeism)
- Do you think the quality of your work has ever suffered because of your drinking?
- Have any of your colleagues or supervisors ever commented on your drinking?
The patient should also be asked if any friends or family members have commented on their drinking. At the same time, a family history for alcohol abuse should be obtained in view of the evidence for genetic predisposition to alcoholism (editorial, Lancet, 1985). Also ask if there is any history of marital discord arising from the patient's drinking. Close relatives should be routinely interviewed whenever possible, since sexual impotence in males, loss of income, and drunken neglect are all painfully apparent to a marital partner, who may often provide the most accurate and believable record of the patient's alcohol drinking history.
Medical Effects of Drinking
The two major indicators of physiologic dependence on alcohol are a history of tolerance to large doses and a history of withdrawal syndrome after a bout of drinking.Physiologic tolerance to large doses of ethanol is a feature of addiction. Just as a narcotic addict can routinely inject a dose of morphine that would kill a normal person, so can an alcoholic appear to function normally (e.g., walk, talk, or drive an automobile) with a level of ethanol in the blood that would render a nonalcoholic unconscious. The question "How much can you drink without getting drunk?" may elicit a boastful and quantifiable response. The ability to drink everyone else "under the table" is commonly perceived as signifying virility and strength, but actually signifies tolerance to an addictive drug and is a major indicator of alcoholism.
Similarly, any history of a withdrawal syndrome is evidence of physiologic dependence on ethanol. Patients should be asked if they have ever experienced an episode of tremor, sweating, hallucinations, epileptic seizures, or delirium tremens ("DTs") while recovering from a bout of drinking. Tremor and sweating alone indicate a mild withdrawal syndrome; a history of delirium tremens indicates that the severity was life-threatening.
Alcohol may adversely affect any organ system in the body. Table 91.2 lists several common and nonspecific symptoms that should alert the physician to the possibility of alcohol abuse.
Alcohol is often abused in combination with sedative hypnotic drugs, and the history should list any concurrent medication with "sleeping pills" or "nerve pills" such as barbiturates or benzodiazepines.
Basic Science
For adults in Western societies, it is a nearly universal experience to drink alcoholic beverages at least occasionally. Ethyl alcohol is by far the most popular recreational drug in the United States and is enjoyed by the majority of drinkers without any observable harm to their health. Nevertheless, approximately 7% of all adults drink to such excess as to become "problem drinkers," and 11% of all deaths are related in some way to the abuse of alcohol. Excessive drinking often leads to an early death; the mortality rate in males may be increased by as much as sixfold (Noble, 1978). Death may result from increased predisposition to suicide, homicide, and fatal accidents, as well as the acute or chronic toxic effects of alcohol on the body. Chronic alcohol abuse predisposes to several diseases, principally hepatic cirrhosis, peptic ulceration, cerebral atrophy, pancreatitis, and cancers of the head and neck (DeLuca, 1981).Clinical Significance
Alcoholism, like syphilis, is a "great imitator"; the symptoms are frequently nonspecific, and it is easy to miss the diagnosis totally unless one routinely screens every patient for the condition. Early diagnosis and energetic treatment can avert many of the medical and social complications of chronic alcoholism and possibly rescue the patient from a premature death. Consequently, devoting a few minutes to routinely and carefully recording the alcohol drinking history may be one of the most useful services a physician can render a patient.Acknowledgment
I thank Daniel Rudman, M.D., and Conrad Swartz, M.D., for their valuable advice and assistance during the preparation of this chapter.References
- DeLuca JR, ed. Fourth Special Report to the US Congress on Alcohol and Health. Washington, DC: GPO, 1981.
- Diagnostic and Statistical Manual of Mental Disorders. 3rd ed [DSM-III]. Washington, DC: American Psychiatric Association 1980.
- Editorial Inborn alcoholism? Lancet. 1985;1:1427–28. [PubMed: 2861540]
- Mayfield D, McLeod G, Hall P. The CAGE questionnaire: validation of a new alcoholism screening instrument. Am J Psych. 1974;131:1121–23. [PubMed: 4416585]
- Noble EP, ed. Third Special Report to the US Congress on Alcohol and Health. Washington, DC: GPO, 1978.
Figures
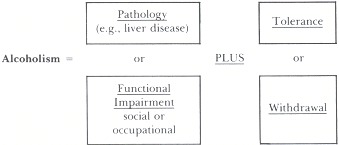
Figure 91.1
Conceptual representation of the DSM-III definition of alcoholism.
Tables
Table 91.1Questions to Elicit Amount of Alcohol Consumption
| Frequency |
 How often do you drink any alcohol? (Every day? Once a month?) How often do you drink any alcohol? (Every day? Once a month?) |
| Under what circumstances? (When stressed or anxious? Only on special occasions like weddings and birthday parties?) |
| How old were you when you started drinking? |
| Location |
| Where do you usually drink? (e.g., In a bar? At parties? Al home?) |
| Quantity |
| What do you usually drink? (Wine? Beer? Spirits?) |
| How much do you usually drink most days? (Attempt 10 quantitate in fluid ounces or liters.) |
| What is the most you might ever drink at any one time? |
| How much do you usually spend on alcohol in a week? |
Table 91.2Symptoms of Alcohol Abuse
| Cardiovascular and respiratory systems |
| Chronic fatigue |
| History of high blood pressure |
| Recurrent chest infections |
| Transient arrhythmias ("holiday heart") |
| Syncope |
| Central nervous system |
| "Blackouts" |
| Memory loss |
| Headaches |
| Depression |
| Numbness and/or tingling in the limbs |
| Seizures (with loss of consciousness, tongue biting, or fecal or urinary incontinence) |
| Difficulty in concentration |
| Gastrointestinal |
| Dyspepsia |
| Loss of appetite |
| Nausea and vomiting |
| Diarrhea |
| Hematemesis and/or melena |
| History of peptic ulcer disease, pancreatitis, or liver disease |
| Genitourinary |
| Loss of libido |
| Impotence in males |
| Musculoskeletal |
| History of recurrent trauma (falls, auto accidents, beatings, etc.) |
Copyright © 1990, Butterworth Publishers, a division of Reed Publishing.
Không có nhận xét nào:
Đăng nhận xét